

Submitted by Dirtperson Steve
Guest Post by A Midwestern Doctor
Big Pharma Has a Remarkably Effective Business Model
Many of you have observed an explosion of RSV (respiratory syncytial virus, a respiratory virus that frequently afflicts children) and to a lesser extent influenza (e.g. a friend called me up today to ask if it was linked to the vaccine and many colleagues have reached out to me about the unprecedented surge they are observing in patients). Although I expected this, it is still somewhat disconcerting to see this happen as RSV is typically not a major concern outside of very specific patient populations.
I first started seeing signs of this concerning trend last year when Australia reported a huge spike in RSV over the summer. This summer, Australia experienced an unprecedented spike in both influenza and RSV. This has led many experts to become worried about the threat we were facing from these diseases and emphasize the urgent need to develop a vaccine for RSV (the last one was pulled because it caused enhanced respiratory disease).
Many vaccines are currently in clinical trials (with vaccines expected to be available next year) and Moderna is presently developing an mRNA vaccine for RSV while Pfizer is opting for a more traditional design. Due to the “emergent” nature of the RSV situation, everyone appears to be going for an accelerated approval which skips the necessary time for the safety testing process, which as the last few years have shown, may not be the best idea when a vaccine already had known safety concerns.
Influenza and RSV Data
One researcher who was working on this question for a concerned colleague was kind enough to put together this wonderful compilation of influenza graphs I was provided with.
Influenza
The next 3 graphs designate the hospitalization rate per 100,000. This is the CDC’s main metric for evaluating the overall consequences of influenza throughout the United States, which I believe it is a reasonable way for doing so. Other metrics such as total influenza cases are highly dependent on testing (like COVID-19 more test automatically produces more cases, and less severity). In these graphs, the red bars represent weeks 40 to 45 of each year and the 2022 rates most likely will increase and peak around January.



Since we are still early in the season, we cannot know for certain that a larger spike will follow later, but all signs point to this happening. For example, beyond the observations mentioned above, consider what happened recently in Australia, as Australia’s experience each year typically predates that of the rest of the western world.
Additionally, as you can see from these graphs, 2020 was essentially a year without influenza. Although this was attributed to lockdowns, a very good case (I agree with) can be made that it arose from influenza and the other many other respiratory diseases that are incorrectly classified as influenza all being rediagnosed as COVID-19.
If we look at the Weekly U.S. Influenza Surveillance Report, we see a similar trend in pediatric deaths (e.g. there are likely the same diagnostic errors for influenza detailed above).


It is too early in the season to know if there is a change, but influenza started earlier this year and is likely to become much worse.
RSV
(This system can be accessed here)

Note: The Y-axis on this graph (ranging from 1.5-4) does not match the overall rate (18) claimed by the CDC, and I am not completely sure why this is as the y-axis seems correct in the other graphs. Nonetheless, the trend in question is still shown.
An identical trend of a massive spike in RSV this year is shown for each age group between the ages of 0-12, although the total number of hospitalizations, as expected, steadily decreases with age (e.g. it is 2.0-4.0 for ages 5-11). The trend begins to shift here:

As the ages increase, the relative spike in RSV also slightly decreases, but until the age of 85 remains elevated (e.g. according to this CNN article, the RSV hospitalization rate for seniors is approximately 10 times higher than before).
At the time of writing, I was unable to locate a dataset demonstrating the trends in death from RSV.
At this point, I can see two potential explanations for why all of this is occurring:
•The COVID-19 vaccines
•Something else (there are quite a few candidates).
COVID-19 Vaccination and Respiratory Diseases
When the vaccination campaign began, many predicted it would lead to an increase in other infectious diseases (there are a variety of explanations for this). I in turn believe that the best candidate to explain what we are observing now are the COVID-19 vaccines.
However, before we proceed further, I need to state that there is a major piece of evidence which argues against it, that being that the increase is also being observed in children between 0-6 months of age, a cohort which the vaccines has not yet been authorized for. Although it is likely some infants in this age range are nonetheless being vaccinated, I am seriously doubtful that enough are being vaccinated to create the effect observed in that age range. In turn I can offer the possible explanations for this inconsistency:
•Something besides the vaccines is causing this spike.
•Vaccine shedding (which I suspect is mediated through exhaled spike protein containing exosomes) from individuals around the infant is mimicking the effects of vaccination.
•Infants have in effect been vaccinated because their mothers were vaccinated.
•Infants are being inoculated with the vaccine through breast milk.
•Immune suppression within the population is causing much higher levels of RSV to circulate, hence increasing the infectious dose children are exposed to (increased infectious doses correlate to a more severe outcome) and possibly creating an internal terrain that creates more pathogenic RSV variants to emerge (immunosuppressed individuals often create harmful variants).
I will now look at the potential reasons why COVID-19 vaccines could be causing an increase in RSV in the other populations.
Direct Immune Suppression
There is a lot of evidence to suggest COVID-19 vaccines (and to a lesser extent the infection itself) cause immune suppression. For example, there have been many cases of individuals developing AIDS-defining illnesses following vaccination (e.g. consider this letter one ICU doc wrote to the H.H.S) and this is something I have also observed within my immediate circle.
On the less severe side of the equation, many have observed the vaccinated appear to be getting sick much more frequently, and in many cases repeatedly catching COVID-19. One of the clearest correlations to immune suppression has been observed in the explosion of both shingles (along with a few other infectious diseases) and severe complications of shingles amongst the vaccinated (Justin Bieber’s recent case of Ramsey Hunt Syndrome is one such example and I provided the evidence clearly linking it to vaccination). This is an important point because developing shingles is classically considered to be linked to immune suppression.
The most concerning example of the link between vaccination and immune suppression regards the explosion of aggressive cancers many have observed (myself included) following vaccination. Recently I compiled a piece with Igor Chudov highlighting the evidence showing this is happening, along with the choice by every responsible party to ignore the clear warning signs and each piece of evidence that suggested otherwise.

Note: Although aggressive cancers are classically associated with immune suppression, they can also be caused by an actively genotoxic agent (which the spike protein has been demonstrated to be and the vaccines themselves are suspected to be). This vaccines caused explosion of cancer is thus likely, but not definitively due to the vaccine immune suppression as a direct genotoxicity could also potentially account for it.
To my knowledge, there are presently three explanations for why the vaccines are immunosuppressive.
The first is that spike proteins kill white blood cells. In patients infected with COVID-19, one of the unusual blood markers you observe is a decrease in white blood cells (typically in systemic infections you see the opposite). Although a human ACE-2 receptor (along with that found in a few other animals) is necessary for the spike protein to enter most cells, COVID-19 and its spike protein through different pathways, is also able to enter and damage or kill many different white blood cells in the body (e.g. see this paper, this paper, this paper, and this paper).
The second is that the spike protein kills the bone marrow, which is responsible for producing blood cells (many of which such as the hematopoietic stem cells are vital for health and proven to decline following vaccination). I was first alerted to this issue when the FOIA’d Pfizer bio-distribution data showed that after being injected, the vaccine accumulates in the bone marrow. Later a patient who required a bone marrow stem cell transplant for cancer told me that he had refused the vaccine because a few people in his online support group who had also gotten this transplant had had it fail after COVID-19 vaccination. Most recently Igor Chudov wrote an article providing evidence that strongly links this form of immune suppression to increasing RSV cases as the body depends upon hematopoietic stem cells (which originate in the bone marrow) to fight RSV.
The third is that the vaccines are causing a general dysregulation of the immune system (particularly the innate side) which results in a decreased ability for it to respond to viral infections and cancers. There are a variety of ways this is occurring, some of which were listed in the above article, hence making listing all of them beyond the scope of this already lengthy article.
There is also one dysregulation not mentioned in that article which likely plays a key role in vaccine immunosuppression. The vaccine provokes a very strong immune response to the body’s own tissue (which is likely a primary reason why they kill people) due to the vaccine being designed to make your own cells be coated with the highly immunogenic spike protein. Although this was a major theoretical concern with the vaccines, Pfizer (and likely Moderna) per leaked regulatory documents, was somehow allowed to exempt themselves from testing the autoimmunity risk (which I inferred was because they discovered it was horrendous and wanted plausible deniability).
This risk has since been demonstrated by the immense spike in autoimmune conditions amongst the vaccinated (honest datasets I’ve looked at have found 20-25% have an exacerbation of a pre-existing condition and I’ve also seen a large number of new autoimmune disorders). A team of German pathologists have done the most detailed work in this area and have demonstrated that tissue of those who were vaccinated have an unprecedented autoimmune response in their tissues that can be fatal. In their most recent presentation discussing these issues, they emphasized another important point: if the immune system is being diverted to attacking its own tissue, it is diverted away from attacking invading pathogens, or put differently this immune dysregulation creates immunosuppression.
In the next section we will further discuss the immunosuppressive consequences of diverting the immune system away to an unnecessary and unnatural topic.
Original Antigenic Sin
The immune system is frequently referred to as the “last frontier of medical science” because so much is still unknown about its workings. This I believe is largely due to the field of immunology adopting a tunnel vision approach guided by their religious faith in vaccines rather than investigating aspects of the immune system which will not lead to a vaccine or immune regulating pharmaceutical.
Because of these biases, there is a general belief that more immunizations are better and that the body can safely and effectively utilize an almost infinite number of vaccinations. In actuality, there is a very finite number of antigens it can respond to, and each vaccination “primes” the immune system to prioritize responding to that specific antigen at the expense of developing an immune response to other antigens. As a result, vaccinated individuals frequently lose varying degrees of their ability to mount an adaptive immune response to new diseases.
This is particularly problematic because most vaccines create an evolutionary pressure that selects for variants not covered by the vaccine (hence why existing vaccines such as the pneumococcal vaccine continually need to be updated with additional antigens and why different boosters such as the bivalent [omicron] COVID-19 booster are often needed).
Most unfortunately, due to OAS, the original vaccine often decreases rather than increases immunity towards the new variant. This has best been shown with those for COVID-19, which I believe is particularly problematic due to the vaccine having a monovalent vaccine targeted to a rapidly mutating part of the virus and the persistence of the mRNA in the system resulting in a prolonged immune stimulation and immune priming to the now extinct spike protein.
Numerous studies have demonstrated previous vaccination increases your likelihood of developing future infections. I believe this has best been shown with the influenza vaccination where it has been shown the vaccination increases your risk of many different respiratory viral infections, including coronaviruses (I also have seen a lot of things suggesting prior influenza vaccination significantly worsens one’s COVID-19 prognosis). Although I was unable to identify any articles demonstrating this for vaccinations besides the failed RSV vaccine increasing the risk of RSV (this is rarely studied), OAS has been a continual concern in RSV vaccine development. In this article on why it was clear from the start that the COVID-19 vaccines could not work and this article on why vaccines consistently fail to prevent disease transmission or herd immunity, I compiled a much more detailed summary of the evidence to substantiate these claims.
However, while I was unable to find studies supporting the link between influenza vaccination and an increased risk of RSV, Del Bigtree was able to uncover that Pfizer and Moderna’s own data admitted this occurred for the vaccine in question!


The entire point of these types of trials is to have data we can extrapolate out to the general population. Sadly that is of course never done when it raises an uncomfortable truth, thus leading to the mystery of why the RSV surge has happened, but I am sure both Pfizer and Moderna recognized the potential market these figures suggested.
Alterations of Communal Herd Immunity
In addition to vaccines frequently failing to live up to their promise of delivering communal herd immunity, they often, unfortunately, do the opposite and alter the natural balance of communal disease transmission, leading to diseases that were previously in a stable balance exploding in prevalence. Put differently, for every action, there is an opposing reaction, and often the unintended consequences of mass vaccination outweigh their intended communal benefits.
The best example of this I know of was seen with the chickenpox campaign (an unnecessary vaccine to begin with as the infection is relatively benign, it has minimal productivity costs to either the parent or child, and it confers a variety of long-term benefits to children such as preventing future deadly brain cancers. After the chickenpox vaccine was launched, a researcher tasked with evaluating the campaign’s efficacy discovered that while it reduced chickenpox, it also increased shingles (a dramatically more problematic infection that results from a reactivation of a dormant chicken pox infection later in life).
When this was investigated, it was concluded to have resulted from a loss of communal boosting from chickenpox infections within the community as a result of the chickenpox vaccination campaign. Despite existing within the scientific literature, all of this, not surprisingly remains relatively unknown and the CDC has shown no interest in investigating it.
Lastly, although I am not an advocate for vaccination, unlike most vaccinations, there is decent evidence showing the shingles vaccine prevents shingles (typically live attenuated vaccinations, while not necessarily safe, are the most effective, so this benefit is unlikely to be seen with the shingles mRNA vaccines being developed by Pfizer and Moderna). I also know numerous people who had recurrent episodes of shingles be treated with vaccination.
On principle, I must admit I am opposed to this approach, as it represents using a vaccine to solve a problem another vaccine created rather than just pulling that vaccine from the market, which synopsizes how much of the pharmaceutical business works (selling pharmaceuticals to “treat” the side effects of other pharmaceuticals). Additionally, there are a variety of other ways to treat shingles (e.g.. ultraviolet blood irradiation, frequency-specific microcurrent). Since there are always contamination issues with live viral vaccines (it’s impossible to grow a clean culture with only one virus) I will always default to utilizing an approach I know is safer, but for many people less privileged than myself, those options are not always accessible and the shingles vaccine may represent their best option for addressing this conundrum.
Note: Only one of the two FDA approved shingles vaccines is a live attenuated vaccine.
The point of that tangent was to illustrate that if the COVID-19 vaccinations significantly worsen immunity to other respiratory viruses, then it is entirely possible that they will also significantly alter their communal transmission and upset a previously established ecological balance of disease infectivity (e.g. the spike we are now seeing).
Mistletoe
Years ago, I was sent a fascinating lecture on anthroposophic medicine in regards to cancer, AIDS, and the workings of the immune system. Like the anthroposophists, I also believe that fevers are critical for health, and many disease result from the fever response shutting down or being suppressed. Mistletoe (a core remedy of anthroposophic medicine due to Rudolph Steiner directly recommending it) is widely utilized for curing cancer and functions by inducing fevers in the body (the Coley’s toxins have a similar effect).

One of the most interesting points I took from his lecture is that the temperature of the body follows a periodic fluctuation in rhythm with the circadian rhythm, and when this rhythm is disrupted or the body becomes too cold, cancer begins. Mistletoe in turn exerts its beneficial effects by restoring the cyclical variability in body temperature, and when that occurs (which happens in the majority of cancer patients receiving mistletoe) it serves as a reliable indicator that the patient will recover from their cancer.
A major curiosity of mine has been if a similar process also occurs in COVID-19 vaccinated individuals (as there are many similarities between them and what the lecturer describes) but unfortunately, I have not yet been able to test the temperatures throughout the day in the vaccine injured. As the lecture is quite long (e.g. one part covers Coley’s toxins, another on how disrupting the pineal glands function through unhealthy light exposures, poor sleep or jet lag) heavily disrupts these vital circadian rhythms, I cut it down to the most important 14 minute segment which can be viewed below:
Other Potential Causes
A variety of other causes have been proposed. Three of these I will focus on in more detail here. The others include:
•A more dangerous variant of RSV emerged (either within immune-suppressed individuals or through deliberate engineering). Although RSV is a respiratory RNA virus (which makes it inherently difficult to produce a vaccine for as it easily mutates), I have not been able to find any papers evaluating the recent changes in RSV genotypes or news articles stating pathologic RSV variants are responsible for the current situation.
•EMFs, some type of spiritual force or collective consciousness moving through the world or some other type of global frequency change (e.g. increased sunspot activity). The advantage of this option is that it provides a means to explain how a change can occur simultaneously around the globe. Although some believe strongly in this hypothesis (e.g. Arthur Fristenberg has shown how many changes in global EMF exposure correlate with significant infectious disease outbreaks and I have had dozens of people ask me if this is what’s causing RSV) I do not believe there is enough to move this hypothesis beyond it being something worth periodically considering. I will note I am very open to the idea EMFs frequently create health problems and I do my best to reduce my exposure (e.g. I do not have WiFi, I have a low EMF smartphone [using /e/ ], I use an air-gapped headset and I live in a very low EMF area), so I have tried to give this theory a fair chance to prove itself.
•COVID-19 infections (especially repeated ones) create permanent damage to the immune system. This one is possible, but it does not explain why it was not an issue in the previous two years.
Moving forward, the three key alternate reasons are as follows:
Lockdowns:
The most common explanation presently being provided for why there is a spike in RSV is that the lockdowns and aggressive social distancing weakened our immune function and ability to develop immunity to viruses such as RSV. There are two major reasons why I object to these arguments.
First, the lockdowns happened very briefly at the start of 2020, and once Biden was elected, many of the remaining COVID-19 restrictions were dropped (there has not been a major change in them in the two years since that time). Despite this, no spike occurred in the previous flu and RSV season (to the contrary no cases were reported). Instead, they only happened this year (e.g. many who experienced this spike were born after the lockdowns ended), which I believe best argues for these events being a result of long-term immune suppression following vaccination.
Secondly, consider the “infamous” Bakersfield doctors who were formally reprimanded by their medical societies after giving a press conference which argued that the lockdowns would create significant immune suppression and increase the likelihood of catching disease. When they raised this argument they were attacked by both the media and the medical profession. Nonetheless, those same parties are now trying to have their cake and eat it by arguing this explains the spike in respiratory infections seen following the vaccination campaign. This is not that different from the explosion in cancers that developed following the vaccination campaign being attributed to missed screening appointments and other routine aspects of medical care (as these were deemed to be non-essential services during the lockdown period).
Not Enough Vaccines:
Recently, like many others here I wrote a well-received critique of the deceptive plea for COVID-19 amnesty (my focus was on her language being dishonest, manipulative and violating certain foundational principles of respectful human communication). Apparently, she struck enough of a nerve to motivate someone with a decent chunk of change to fly this banner around her house:

After I looked into her more, I discovered she had a large substack following for her “evidence-based” parenting newsletter and likely made quite a bit of money from this story promoting her to new subscribers. I am thus hesitant to contribute to her publicity efforts, but I could not help but notice her recent “evidence-based” article on how to prevent illness this Thanksgiving and prevent your child from getting RSV. Her advice consisted:
•Test as much as possible.
•Wash hands as much as possible.
•Socially distance your child in rather extreme ways.
•Get the COVID-19 booster.
•Get the annual influenza vaccine.
As much as I want to criticize her, I must recognize that her advice is what the CDC and many others almost always universally recommend for the every respiratory virus, even though at least in the case of the flu it has had to change in the likelihood of being severely afflicted with the disease. One of the best arguments against these policies can be shown by this graph. Keep in mind, although we have continually increased how many annual flu shots are given in the United States (e.g. 12 million in 1980 to nearly 200 million in 2020), nothing we have done has had a meaningful impact on influenza.
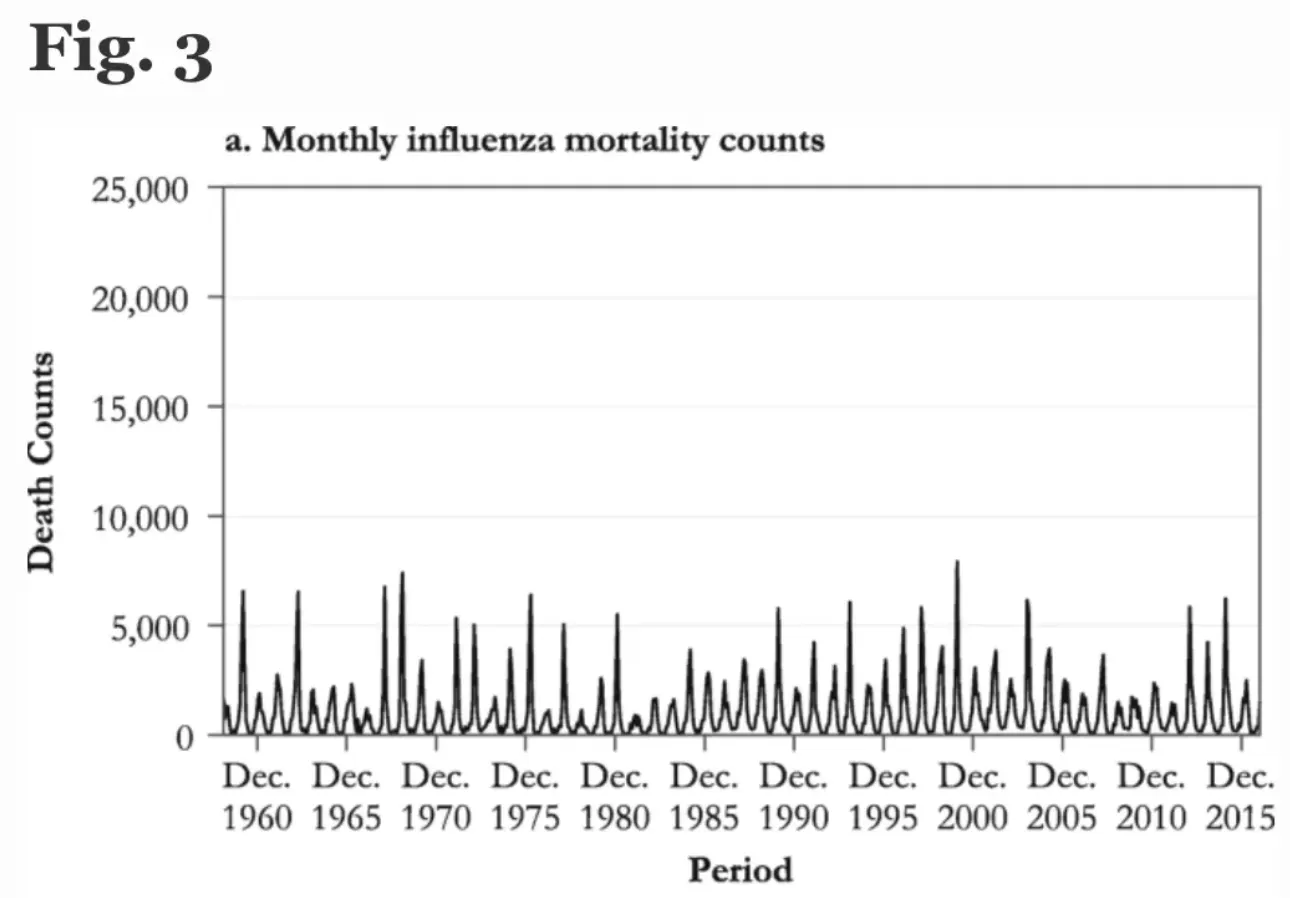
As you can see, although there is allegedly an amazing benefit from this program that somehow outweighs the myriad of issues associated with this vaccine, it is somewhat difficult to discern what that benefit is. Nonetheless, many like Oster, believe that getting your annual vaccinations is the best protection we have against RSV despite there being no mechanism for this and the vaccine frequently increasing your risk of getting respiratory viruses such as COVID-19 and RSV.
Although this section appears to be in jest, many already believe the reason we are having an RSV spike is because there is not a vaccine against it, and once it gets fast-tracked by the FDA will insist that those who refuse the RSV vaccine are the ones who are actually responsible for the “deaths from RSV.”
Misdiagnosis
Every year, there are a relatively similar number of individuals who die in the hospital from respiratory viruses (in certain years there is also a spike). One disingenuous thing certain departments of the H.H.S. (e.g. the CDC) do is reclassify those deaths as influenza deaths so that as much hysteria about the flu as possible can be created each year to sell flu shots and used to obtain congressional funding for their department.
In actuality, many of those deaths are from something besides the flu (e.g. a different respiratory virus) or were unrelated to the infection (e.g. they would have died anyways and incidentally had a positive influenza test). I tried to cover this in more detail here, including citations of papers from top medical journals which emphasized that public health officials consistently make disingenuous claims about the influenza vaccines they promote as very little evidence exists that they work and that there is a widespread failure to differentiate between respiratory viral infections caused by influenza versus another respiratory virus.
A common question I frequently encounter on this topic is “if you believe that, then why do you think COVID-19 existed?” My answer is that COVID-19 was a highly unique and dangerous disease that at a few times caused a spike in overall mortality, but because there were large financial incentives for healthcare providers and hospitals to classify everything as COVID-19, many diseases, including the annual respiratory viruses, were erroneously diagnosed as COVID-19 when they should not have been.
One of the better quotes I’ve found on our present situation can be found here:
The average for daily new Covid cases in the US has remained below 50,000 since early October, less than the 80,000 average daily for this time last year, Centers for Disease Control and Prevention data show. However, public health groups and Biden administration officials have warned a wave of new cases could come this winter and that current Covid case counts could be missing those who only use at-home tests.
Another way of wording this is that COVID-19 “rates” are in many ways an arbitrary metric proportional to how many people are being tested (which goes back to a key point…testing should not be done in asymptomatic individuals because the results are largely meaningless). Now that routine testing has resumed for influenza and RSV, those diseases are also thus increasing in incidence.

However, at the same time, I do not believe the current wave of RSV is a result of diagnostic misclassification, as it is clear to me that what we are seeing now is not something that has been observed before (e.g. in addition to hospitalists reporting this, a few doctors opposed to vaccination who do not follow the conventional narrative have also reported this trend to me).
My best guess was that early on, certain vaccine companies recognized that the COVID-19 vaccines were going to cause RSV to turn into a problem and decided to address this issue by developing RSV vaccines (even though after decades of research a successful vaccine for RSV has not yet been developed). Now that the COVID-19 vaccination market is beginning to dry up (because of how clearly they have failed, much of the public recognizes they are a scam and is unwilling to get additional boosters), the industry is attempting to pivot to selling RSV vaccinations.
It should be noted that Pfizer put out a press release on November 1st regarding the positive results of their phase 3 RSV vaccine trial. Since that time, the media coverage regarding the threat of RSV has exponentially increased, which is not that different a situation from when a previous positive trial result for Pfizer’s alopecia drug was followed by a perfectly tailored “incident” at the (Pfizer-sponsored) Oscars which put Pfizer’s disease into the media spotlight. It should also be noted that the current alarming script being used (hospitals are being overwhelmed and patients are having to be treated outside of the typical hospital rooms) to describe the RSV pandemic has been reused more times than I can count for both COVID-19 and Influenza and is largely a product of the hospital beds available for these issues being chronically understaffed.
Because of all of this, while RSV has already become a real issue for many, an effort is also being made to hype up the severity of the disease (e.g. inflating case numbers with inappropriate testing, lots of media coverage being given to the issue). If this proves successful, it will once again become possible to fast-track the approval of an unsafe vaccine, which will likely have many issues, although I am doubtful they will be as bad as those observed for the spike protein gene therapy vaccines.
Conclusion:
A month and a half before the midterms, Joe Biden “ended” the pandemic, and then not long after, instead renewed his state of emergency. One of the rules of Government has always been that those in power will not voluntarily relinquish any power they have gained, and it is my sad belief that at least half of our government has gotten addicted to the power public health emergencies give them.
For example, the governor of Colorado, feeding into a narrative of a disastrous triple epidemic season recently declared an “emergency” for not only COVID-19 but also RSV and Influenza. To my knowledge, there has never been a public health emergency for RSV (please correct me if there was).
Much more concerningly, following the World Economic Forum’s advice, all 20 leaders at G20 signed a pact for their countries to require a global vaccine passport be utilized for international travel (Schwab of course attended). There are a variety of serious concerns over a vaccine passport being implemented and it is not something that should be decided by a private group above the government of each nation (especially since many citizens have made it clear they do not want it). Taking this further to extremes, I have heard from friends in China (where a cell phone is required to access virtually every service) that presently unless you are tested for COVID-19 every two to three days (depending on the local case numbers), you denied access to virtually every service in the country.
Power is addictive, and once it is gained, those who have it will always push for more. Most likely, we will see the same “mistakes” that occurred over the last few years repeated again and again into the future (hyping up infectious diseases to support the government, banning all effective treatments which threaten this newfound power base, promoting or mandating a variety of ineffective and harmful vaccines, etc.).
Because power is addictive, like addicts, those in charge will often be willing to go to attack anyone who gets in the way of what they are doing. As many are starting to awaken to the pandemic scam, this is creating a serious challenge for the political leadership. Robert Malone recently gave a short but important talk on this subject and what is critical for us to do moving forward so we do not end up in the world these people have dreamed of.
Similarly, many doctors I knew who were previously pro-vaccine have lost their faith in the COVID-19 vaccines because they along with many others they knew caught COVID-19 multiple times after being vaccinated or boosted. This red-pilling experience has made them open to looking at the harms and many have also begun to share very concerning trends they have seen (e.g. a neurologist a colleague spoke to at a prestigious hospital shared that they were seeing multiple cases of Myasthenia Gravis onset after vaccination each week, an autoimmune condition a close colleague informed me they had also observed worsen after vaccination).
A central argument I have made here (most thoroughly discussed in this recent article on the causes and treatments of Alzheimer’s disease) is that there has been a steady decline over the last 150 years in the health and vitality of the human species which often suddenly “jumps” and some of those jumps I believe directly resulted from vaccination (e.g. the smallpox vaccine being mandated on humanity, and the 1986 vaccine act which exempted manufactures from liability and birthed the modern explosions of new vaccines being added to the immunization schedule). Interestingly, building upon the observations with mistletoe described above, gradual decline in the average body temperature of Americans has been observed over the last 200 years (note: body temperature also declines as you age).
Since the COVID-19 vaccinations started, I have had the fear that like many of those before me, I am one of those present to bear witness to a fundamental change in the health of the human species. It is thus my hope that this spike in respiratory diseases is not a sign of what is to come.
Unfortunately, the pharmaceutical industry is incentivized to create this issue as they are paid for each “treatment” they sell over and over to the same customer, not each cure they produce or if their product creates a net benefit to each recipient. Although many regulators exist to prevent this from being a problem, the industry has solved this issue by paying them off to cooperate, and because those corrupt officials have met a critical mass, those with integrity who do not wish to comply are typically fired or reassigned to areas where they have no influence on the drug approval process. I don’t know what can be done to fix this, but I hope through these writings I can at least do a bit to bring attention to the issue.
It is my sincere desire to provide readers of this site with the best unbiased information available, and a forum where it can be discussed openly, as our Founders intended. But it is not easy nor inexpensive to do so, especially when those who wish to prevent us from making the truth known, attack us without mercy on all fronts on a daily basis. So each time you visit the site, I would ask that you consider the value that you receive and have received from The Burning Platform and the community of which you are a vital part. I can't do it all alone, and I need your help and support to keep it alive. Please consider contributing an amount commensurate to the value that you receive from this site and community, or even by becoming a sustaining supporter through periodic contributions. [Burning Platform LLC - PO Box 1520 Kulpsville, PA 19443] or Paypal
-----------------------------------------------------
To donate via Stripe, click here.
-----------------------------------------------------
Use promo code ILMF2, and save up to 66% on all MyPillow purchases. (The Burning Platform benefits when you use this promo code.)

It was the vaccine.
FIFY.
You don’t want to kill granny, do you?
Hold my beer and hand me that cross stitched sham.
TCS-
No way. Catholic Girls caused it, at the CYO.
Of all people, you should know.
You might have a point. Those bitches never confess.
it’s not like RSV was never around before this year,…it’s always been there, and it’s opportunistic like any other pathogen. If your immune system is compromised, then you are more likely to pick up whatever is floating around. It’s not rocket science.
Moron Stream Media
Let’s see if I can summarize:
Huge numbers of people are going to die from the incessant efforts to keep anyone from dying**.
…
** of things that, really, not all that many people would die of if “the experts” had just left things alone.
But, hey, millions dead would be worth it if it saves just one life … right?
But they mean well.
It could be worse, were they to die naturally in the due course of time and tide.
Just think of all the new fertilizer that will be available at next to zero cost.
” new fertilizer that will be available at next to zero cost”
Chock FULL of Heavy Metals, Hormones, and various ‘Pharmaceuticals’.
FLAME will Purify. Eventually. And Then?
Revelation 21:1 “And I saw a new heaven and a new earth: for the first heaven and the first earth were passed away; and there was no more sea.”
As the chapter opens, all the sinners of all the ages, both demons and men, including Satan, the beast and false prophet, are in the lake of fire forever. The whole universe has been destroyed, and God creates a new universe to be the eternal dwelling place of the redeemed.
“A new heaven and a new earth”: The entire universe as we now know it will be destroyed (2 Peter 3:10-13), and be replaced by a new creation that will last forever. This is a Old Testament reality (Psalm 105:25-26; Isa. 65:17; 66:22), as well as a New Testament one (Luke 21:33; Heb. 1:10-12; see note on 20:11-15).
“There was no more sea”: Currently three-fourths of the earth’s surface is water, but the new environment will no longer be water based and will have completely different climatic conditions (see notes on 22:1-2).
But the day of the Lord will come as a thief in the night, in which the heavens will pass away with a great noise, and the elements will melt with fervent heat; both the earth and the works that are in it will be burned up (2 Pet. 3:10).
“A new heaven and a new earth”: The “new heaven” is the atmospheric heaven around and above the earth.
This area has been the domain of Satan (see Eph. 2:2), and must be purified before the heaven of God can come down to the new earth. This new earth will be a perfect environment similar to that of the Garden of Eden. A unique distinction of this new earth will be that the vast oceans of water that now cover three fourths of the world’s surface will not be included, leaving much more habitable land for the population of the redeemed.”
STFU; mask up; lock down; get “vaxxed”; get “vaxxed again; get ” boosted”; get “booster again; get boosted for a third time…and don’t you EVER question the “Psyience “*, serf.
of course destroying bone marrow and WBC is how it is supposed to work.
*Psyience ( C)copyright and TM Aunt Acid 2022.
The CDC lied and children died: Now come the lawsuits
Rochelle Walensky continued to cite debunked study after it was exposed as a fraud
https://www.naturalnews.com/2022-11-24-cdc-lied-children-died-now-come-lawsuits.html
Lets say you eventually win those lawsuits? Who will you pass the money to? Big Pharma. I have to fix my problems with more pfizer drugs. Good thing I vaxxed my kid too. I got the money I got the money yes compen’sesh….. Umm, aren’t you angry your kid died? “Nope I’m angry I spent the other half of my payout buying mdma for kids at alameda”.
Kinda baffles me when I see a study that references CDC data.
All it took was “won’t be held liable” for me.
That’s all it should have took.