


Dorothea Lange 4 families, 15 children, from Texas Dust Bowl, in roadside camp, Calipatria, CA Mar 1937
Ebola was until a few weeks ago mostly a forgotten affliction in the western world. Something that flared up in the Congo or thereabouts, parts of the world we’re aware of only because of the horrors of machete attacks and other mayhem induced by our own secret services in order to keep ‘our’ access to their mind-boggling amounts of resources going, while their populations live in conditions many miles below squalor.
We have applied divide and rule in the Congo better, or more ferociously, depending on your point of view, than anywhere else, ever. Hardly a word about western cruelty seeps through to our own media. A true imperium success story.
But the present ebola epidemic is not taking place where the disease was mostly raging. It’s in western Africa now. Where immense segments of native forest have been cut down, which in turn brought long-time ebola carrying fruit bats closer to other animals, and in turn to humans long dependent on bushmeat for survival.
Somewhere in that chain of events it was probably inevitable that an epidemic would break out. Of ebola or any other of a long list of viral or bacterial diseases. It’s also inevitable that a next epidemic will follow.
Until recently, my own personal knowledge of ebola was limited to the idea that it was one of, if not the worst way for a human being to die. Intense internal bleeding will do that. Something I find sorely missing in western media coverage of the people dying by the side of the road in west Africa. How they’re dying, that is.
It’s treated in a very detached way, as if it doesn’t really concern us until it might spread our way. ‘Western’ cases get treated with experimental drugs, while 4000+ Africans so far have been left to perish by the side of dirt roads in excruciating pain.
The ones that did receive treatment were attended to by local doctors, and that has led to dozens of the best and bravest doctors in Sierra Leone and Liberia succumbing to ebola themselves, a major feat in countries where per capita access to a doctor is mostly a tenth or a hundredth of what it is where we live. Take away doctors out of that situation, and that’s not even including nurses, and you have a disaster on your hands.
I’m not an expert on ebola or infectious diseases in general by any means, but I can read, and I can think, and occasionally I manage to bo both simultaneously. And what I see so far is a sweet mix of complacency, denial, stupidity and human error.
There’s a lot of political interest in downplaying the danger ebola poses. There’s even more economic interest in doing that, but then the two are Siamese twins. As of today in America, and last week in continental Europe, that attitude has become a threat to potentially millions of people.
I saw someone comparing HIV deaths to Ebola deaths, with the intent to downplay the threat, 1 million HIV deaths, ‘only’ 4000 ebola deaths. But ebola’s just getting started, and it’s much more contagious. Which makes such comparisons as irrelevant as it makes them dangerous.
The first Ebola infection on US soil that was announced today developed in the exact same way the one in Spain last week did: a health care worker tending to a confirmed ebola case got him/herself infected. Both ’2nd generation’ cases have no idea how they were infected. The US nurse was allegedly wearing full-body protective gear all the time, while the Spanish nurse herself said she had no clue how she could have gotten the disease.
In the US case, we know that the first deadly victim, Thomas Duncan, had been in Liberia. He was sent home by several medical services after both reporting symptoms, and stating he’d been in ebola infected territory.The very same thing happened to the Spanish nurse, who was sent away from at least 3 clinics with a Tylenol prescription, after she had said she’d been attending to an ebola patient.
The patient she had been nursing was a priest who had been flown in from Africa after exhibiting symptoms. He was, however, the second Spanish priest in that situation. The first one reportedly died in the same hospital in Madrid as long ago as August.
Madrid got a lot of flack for the infected nurse: it was accused of not having its precautions properly in place. We should now review how well the Texas Presbyterian is doing in that regard. Given the fact that the Texas nurse diagnosed, or rather confirmed, today, was allowed to lead a normal personal life, socializing, shopping etc., until (s)he started exhibiting obvious symptoms, should make us feel queasy.
There will always be plenty political voices more than willing to declare that ‘there is no need to panic’ or ‘now is not the time to panic’, but we need to realize that what politicians and media say is inevitable based on economic grounds.
It might be worth contemplating to isolate western Africa from the rest of the world, halt flights etc., and meanwhile give them all the support we can, no matter what the cost. We choose instead to do everything related to support on the ground on the cheap, bleeding WHO coffers dry while we’re at it, and we let transportation options continue, because it would cost ‘too much’ not to. Money will rule our approach to ebola, like to everything else, until it’s too late.
Ironically, it was George W. Bushmeat government’s bio-terrorist anthrax and flu paranoia in the wake of 9/11 that injected a lot of money into America’s epidemiology protection layers. If not for those paranoid billions, I kid you not, G-d help us. His epitaph will read not only that he was an accomplishes portrait painter, he may well also have saved America from a much worse epidemic than it’s yet to get. America could sure use some of that paranoia right now.
And so could Europe, where everyone to a man solemnly declares that the chances of ebola appearing in their country are slim to none. And where dozens of flights arrive daily from west Africa. To paraphrase the CDC’s Mike Osterholm: the virus moves at virus time, we move at bureaucrat time.
The nurse is Madrid is reportedly healing, she’s been given the experimental ZMapp drug. We better get a million doses of that to Liberia and Sierra Leone. But we’ll probably fight over the economics of that until we need 10 million doses.
We’ve maybe grown so accustomed to living in a casino economy that we think the world is a crap table. But some things had better not be wagered on. Remember the Spanish Flu. Or should I say: Remember the Spanish Flu? Again, we tell ourselves no major epidemic could hurt us. We understand viruses as poorly as we do the exponential function. Which happen to have lots in common.
Judging from what we’ve seen so far, our health care systems are woefully unprepared for even single cases of ebola infection occurring on our soil. What’s going to happen when there’s dozens? Are we just going to say that there’s ‘only’ a 25% chance of that, based on some computer model? Or are we going to make sure we do what we can to keep ebola away from our lands?
There’s only one way to make sure: get into western Africa now, with all we have. Good for us, and good for our karma.

” ….. while 4000+ Africans so far have been left to perish by the side of dirt roads in excruciating pain.” ——— from the article
Well, I hope they build better roads, then.
Don’t allow flights in/out of that section of Western Africa.
Have the Army Corps of Engineers build some Popeye’s Chicken Shacks. Then we air drop chicken and watermelons as a humanitarian effort.
“Don’t allow flights in/out of that section of Western Africa.” —– Dutchman
BINGO!
***** BREAKING NEWS … occurring NOW *******
BOSTON —Medical crews in hazmat suits responded to an arriving plane at the international terminal at Logan Airport Monday afternoon. A Massport spokesman told NewsCenter 5 that five passengers on board an Emirates flight had become sick with flu-like symptoms.
.
http://www.wcvb.com/news/medical-crews-surround-aircraft-at-logan-airport/29093968
The people on the flight shouldn’t have ordered the ebola burgers.
Seriously. Have you eaten airplane food? If they quarantine every flight where people feel sick after eating that crap, there won’t be any planes in the air.
By the way, airline stocks are down 7% in the last three days.
According to a comment on Zerohedge.com, the Russians will have a vaccine ready to send to Africa in two months. From the rt.com website:
“In two months, Russia is planning to send a new experimental vaccine against Ebola to Africa, according to the country’s health minister. The efficiency of the drug, which is to be tested on the ground, is about 70-90 percent.
Today we are discussing that we will have enough of Triazoverin vaccine in two months so that we can send them to our personnel in Guinea and test its efficiency in clinical conditions,” Health Minister Veronika Skvortsova said.
The vaccine has so far proved efficient against various hemorrhagic fevers, including the Marburg virus which is very similar to Ebola.
“The efficiency ranges between 70 and 90 percent and this is a very good indicator,” Skvortsova said.”
http://rt.com/news/195536-ebola-russia-vaccine-send/
“By the way, airline stocks are down 7% in the last three days.” ——- Admin
Would you advise us to buy the dip? Is now the best time to buy?
Buy when there is blood in their eyes.
I guess Ebola is airborne. The dreaded bug arrives via modern aviation.
Shut the freaking planes down now.
[img [/img]
[/img]
Don’t worry people!!!
Obola has a handle on Ebola
[img [/img]
[/img]
Ok, now THIS is worrisome!
http://www.politico.com/story/2014/10/ebola-chocolate-industry-africa-effects-111809.html
[img [/img]
[/img]
Is it me, or does it seem to others that the Fedgov seems unable to arrive at even the most common sense solutions to problems. Like shutting down air traffic from countries with a raging epidemic? It’s worse than Katrina all over again.
Stucky,
In Boston, they will get top flight care without regard to the cost, even if they are here illegally or if they lied about their circumstances surrounding where they came from. Our attorney general now running for governor stated and I quote ” Technically it is not illegal to be illegal in Massachusetts” with regard to being an illegal alien.
http://www.youtube.com/watch?v=jRiXYvsrGV4
I would go back up on the roof but it is dark and time to make dinner.
Bob.
Too bad for West Africans. Isolate the place and let Ebola burn itself out. Nothing else we can do. The idea that the United States is morally compelled to solve every problem in the world is ridiculous. And send back the African “immigrants” who have been allowed to slither into the U.S. thanks to the Democrats and the 1965 immigration law.
[img [/img]
[/img]
If the number of Ebola patients in the US continues to increase I predict a mass refusal of nursing staff to care for them. As a nurse myself I sympathize. There’s no patient anywhere who’s worth my life, nor the lives of my family members. I have a license and calling, not a death wish.
About 70 hospital staffers cared for Ebola patient
Associated Press
By MARTHA MENDOZA
DALLAS (AP) — They drew his blood, put tubes down his throat and wiped up his diarrhea. They analyzed his urine and wiped saliva from his lips, even after he had lost consciousness.
The size of the medical team reflects the hospital’s intense effort to save Duncan’s life, but it also suggests that many other people could have been exposed to the virus during Duncan’s time in an isolation unit.
On Monday, the director of the Centers for Disease Control and Prevention said the infection of the nurse means the agency must broaden the pool of people getting close monitoring. Authorities have said they do not know how the nurse was infected, but they suspect some kind of breach in the hospital’s protocol.
The medical records given to the AP offer clues, both to what happened and who was involved, but the hospital said the CDC does not have them.
A CDC spokeswoman said the agency reviewed the medical records with Duncan’s care team and concluded that the documents were not helpful in identifying those who interacted directly with the patient.
“This is not something we can afford to experiment with. We need to get this right,” said Ruth McDermott-Levy, who directs the Center for Global and Public Health in Villanova University’s College of Nursing.
Until now, the CDC has been actively monitoring 48 people who might have had contact with Duncan after he fell ill with an infection but before he was put in isolation. The number included 10 people known to have contact and 38 who may have had contact, including people he was staying with and health care professionals who attended to him during an emergency room visit from which he was sent home. None is sick.
The CDC has not yet established a firm number of health care workers who had contact with Duncan.
“If this one individual was infected — and we don’t know how — within the isolation unit, then it is possible that other individuals could have been infected as well,” said Dr. Tom Frieden, director of the CDC. “We do not today have a number of such exposed people or potentially exposed health care workers. It’s a relatively large number, we think in the end.”
Caregivers who began treating Duncan after he tested positive for Ebola were following a “self-monitoring regimen” in which they were instructed to take their temperatures regularly and report any symptoms. But they were not considered at high risk.
Typically, the nurses, doctors and technicians caring for a contagious patient in isolation would be treating other people as well and going home to their families after decontaminating themselves. The hospital has refused to answer questions about their specific duties.
The 1,400-plus pages of medical records show that nurses, doctors and other hospital employees wore face shields, double gowns, protective footwear and even hazmat suits to avoid touching any of Duncan’s bodily fluids. Ebola spreads through direct contact with those fluids, usually blood, feces and vomit. The virus has also been detected in urine, semen and breast milk, and it may be in saliva and tears.
CDC officials said there were chinks in that protection at Texas Presbyterian, but they have not identified them and are investigating.
“Patient had large, extremely watery diarrhea,” a nurse wrote in a report filed the day Duncan tested positive.
Another nurse noted that Duncan’s urine was “darker in color with noted blood streaks.”
View galleryGraphic shows how to carefully remove protective gear …
Graphic shows how to carefully remove protective gear used when treating ebola infected patients; 3c …
It was unclear from the records released to the AP how many of the approximately 70 individuals involved in Duncan’s care had direct contact with his body or fluids.
Dr. Aileen Marty, a World Health Organization doctor who recently returned to Florida International University after a month fighting Ebola in Nigeria, said no amount of protection is going to help if hospital workers do not put on and take off their protective layers carefully.
“The first thing in caring for someone with Ebola is to do everything in your power to never become a victim,” she said.
And tracking all contacts, even within the medical setting, is complicated.
Generally, the first step in locating care providers for isolated infected patients is a personnel log on the door, “that should have everyone going in and out, signing in and out,” said Dr. Lisa Esolen, Geisinger Health System’s Medical Director of Health Services and Infection Prevention and Control. Medical records indicate the Dallas hospital had a log.
On the day before Duncan died, records indicate that at least nine caregivers entered and exited the room.
A spokesman for Texas Health Resources, the hospital’s parent company, said the CDC probably has a log from the room door that would list everyone who got close to Duncan.
Dr. Christopher Ohl, who heads Wake Forest Baptist Medical Center’s infectious-disease department and has worked with the CDC in the past, said the expanding monitoring “is an abundance of caution that’s probably beyond what needs to be done” because medical caregivers will notice if they’re getting a fever, and they’re not contagious until that point.
“You start to know when you get those body aches and headaches, most people know that,” he said. “It’s not like you’re surprised by it. Most people can figure out what to do when that happens.”
___
Associated Press writers Maud Beelman and Jamie Stengle contributed to this report.
There’s no patient anywhere who’s worth my life, nor the lives of my family members -Susan
Yanno, Suz, I understand that. I have worked at many an airfield and often times, alone, some days I put my life at risk crawling atop horizontal stabilizers, under a jet engine, which could suck my sorry ass in, and working with hydraulic pressurized control surfaces exceeding 3000 psi at the actuator. I signed off on many a log book certifying an aircraft safe for flight. That was my job to make the public safe.
Ebola, fuck you, just fuck you, I aint gonna go crawl in a corner in fear.
Map: Where Ebola is likely to go next
Ebola already reached the US when a patient was diagnosed in Texas on September 30. But where is the disease likely to go next? A map from MOBS Lab and Northeastern University shows the risks:
[img/cdn3.vox-cdn.com/uploads/chorus_asset/file/2344418/risk_of_ebola_spread.0.png) [/img]
[/img]
o develop these estimates, researchers used a computer model that tracks the frequency of international traffic to different countries, the progression of the disease in already affected countries, and the incubation time and other aspects of Ebola. The estimates will be updated as the epidemic continues.
Outside of Africa, the risk is relatively high in the UK and France, but thankfully very low in India and China. The more advanced health-care systems in the UK and France are much better equipped to deal with an Ebola outbreak, while less advanced systems in China and particularly India, which also have considerably bigger populations to manage, could struggle to deal with an epidemic.
Peter Piot, who helped discover and name the virus, told the Guardian about his concerns with an outbreak in India:
But an outbreak in Europe or North America would quickly be brought under control. I am more worried about the many people from India who work in trade or industry in west Africa. It would only take one of them to become infected, travel to India to visit relatives during the virus’s incubation period, and then, once he becomes sick, go to a public hospital there. Doctors and nurses in India, too, often don’t wear protective gloves. They would immediately become infected and spread the virus.
http://www.vox.com/xpress/2014/10/13/6959103/ebola-spread-international-epidemic-china-india-europe
18 things you need to know about Ebola
Ebola has infected 8,000 people and could infect 1.4 million by January
http://www.vox.com/cards/ebola-facts-you-need-to-know/what-is-the-ebola-virus#E6723144
Map: Where Ebola is likely to go next
Ebola already reached the US when a patient was diagnosed in Texas on September 30. But where is the disease likely to go next? A map from MOBS Lab and Northeastern University shows the risks:
[img/cdn3.vox-cdn.com/uploads/chorus_asset/file/2344418/risk_of_ebola_spread.0.png) [/img]
[/img]
o develop these estimates, researchers used a computer model that tracks the frequency of international traffic to different countries, the progression of the disease in already affected countries, and the incubation time and other aspects of Ebola. The estimates will be updated as the epidemic continues.
Outside of Africa, the risk is relatively high in the UK and France, but thankfully very low in India and China. The more advanced health-care systems in the UK and France are much better equipped to deal with an Ebola outbreak, while less advanced systems in China and particularly India, which also have considerably bigger populations to manage, could struggle to deal with an epidemic.
Peter Piot, who helped discover and name the virus, told the Guardian about his concerns with an outbreak in India:
But an outbreak in Europe or North America would quickly be brought under control. I am more worried about the many people from India who work in trade or industry in west Africa. It would only take one of them to become infected, travel to India to visit relatives during the virus’s incubation period, and then, once he becomes sick, go to a public hospital there. Doctors and nurses in India, too, often don’t wear protective gloves. They would immediately become infected and spread the virus.
http://www.vox.com/xpress/2014/10/13/6959103/ebola-spread-international-epidemic-china-india-europe
18 things you need to know about Ebola
#7 Ebola has infected 8,000 people and could infect 1.4 million by January!!!
How bad could the Ebola outbreak get? There are lots of predictions floating around. The World Health Organization projects that 20,000 people will be infected in November
But there are fears that the supplies and health-care workers needed to bend the epidemic curve downward and save lives won’t reach Africa quickly enough. Doctors need to be trained. Hospitals need to be built. Many suspect that there has been widespread under-reporting of actual Ebola cases, since people have been turned away from overflowing hospitals and others have been hiding in their homes, afraid that coming out with Ebola will mean they never see their families again or that they are ostracized by their neighbors.
Assuming the worst is true, the Centers for Disease Control and Prevention has a much bigger projection for this epidemic: up to 1.4 million people infected by January.
1 What is the Ebola virus?
2 How do you catch Ebola?
3 This is what it feels like to have Ebola
4vEbola is in the United States for the first time
5 The CDC is trying to ensure Ebola doesn’t spread in the US
6 Ebola has never spread to this many countries before
7 Ebola has infected 8,000 people and could infect 1.4 million by January
8 We have no idea how bad the Ebola outbreak actually is
9 Poverty is one big reason why Ebola is spreading so quickly
10 Health-care workers are dying in record numbers
11 One problem with treating Ebola is that Ebola treatment is draconian
12 Global health agencies were too slow in responding to the Ebola crisis
13 The worse the outbreak in West Africa, the more global spread
14 There’s no cure for Ebola
15 The US is now frantically racing to find an Ebola treatment
16 The majority of Ebola deaths may not be from Ebola
17 The US and other countries are treating Ebola as a “security risk”
18 Ebola is tearing apart West Africa’s social fabric
18 Cards / Edited by Julia Belluz Updated Oct 13 2014, 3:10 pm
For the 18 things you need to know about Ebola go to VOX
http://www.vox.com/cards/ebola-facts-you-need-to-know/what-is-the-ebola-virus#E6723144 or
http://www.vox.com/cards/ebola-facts-you-need-to-know/its-the-worst-ebola-outbreak-on-record#E6723144
[img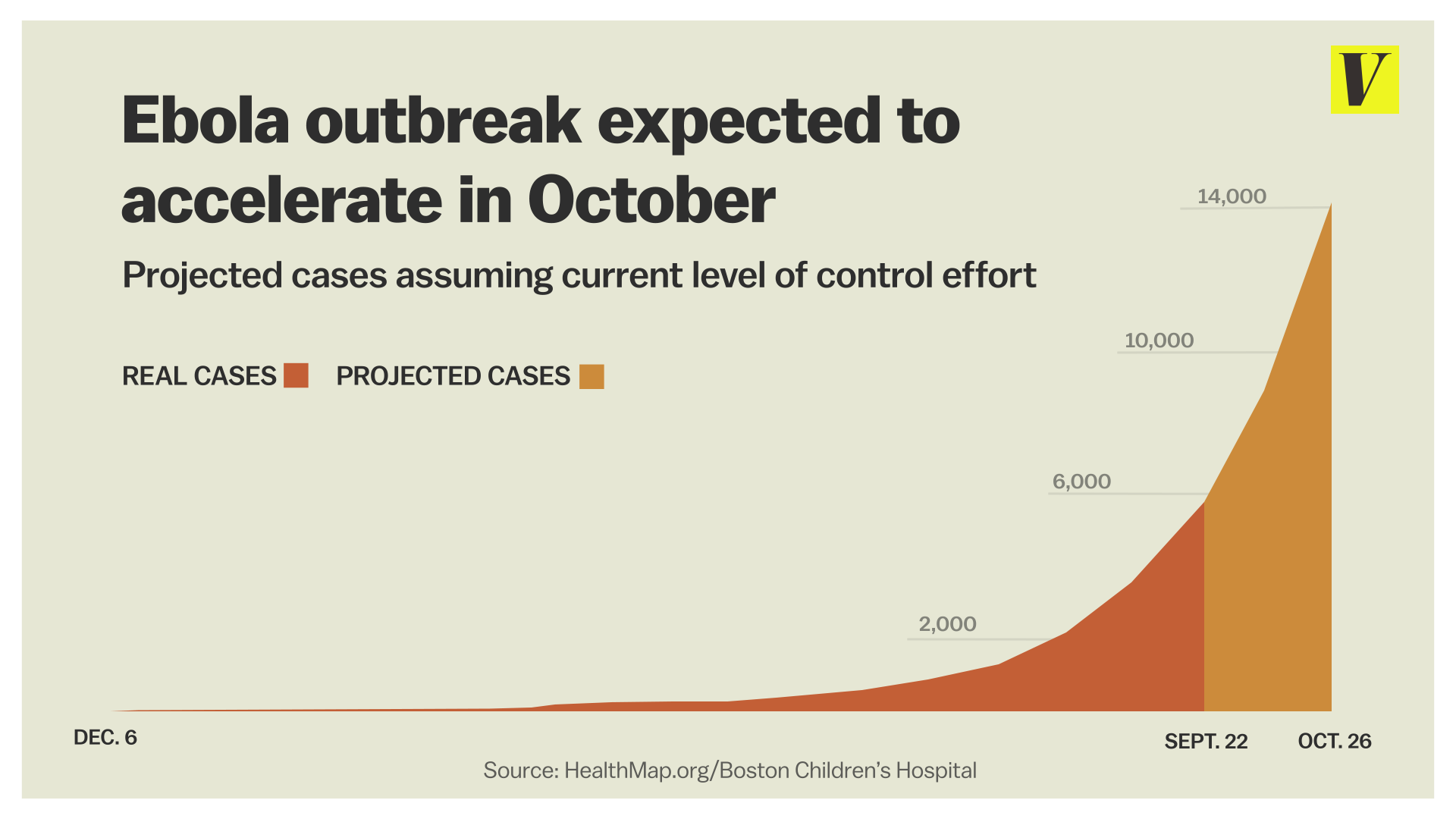 [/img]
[/img]
Extrapolation is a wonderful technique. Is this a chart of the U.S.?
I believe the epidemic did not stay contained in Africa because certain countries were so gleeful to throw money at any village that had infected that they were being ‘fabricated”. Yeah! here’s your grant money. And while REAL illnesses were not contained by our extremely mobile society and the slums of African countries which give rise to increased infectious rates – (along with the eating bushmeat because there is no farming and the aid food goes to the warlords)
AND, while villages used to self-quarantine, now guards can be bribed to let certain people out, as well as military getting certain people out (politicians) to spread the disease further.
Just read on ace of spades and have been reading raconteurreport.blogspot.com that
we’re not ready for this, by any means. And the nurse’s boyfriend has now been hospitalized. How many people did HE come in contact with?
The protocol for treateing obola is LEVEL FOUR equipment, not the paper masks and paper gowns that they have been showing. even if they DO have eye and face protection on. This affects mucous membranes.
anybody else read the chilling article on altmarket about infecting n. american animals so that they are carriers? obola will no longer be a pandemic limited to Africa anymore.
On a positive note, if this takes down 1-2% of the population, society won’t collapse that fast. Most of them are expendable anyway. I mean, only when the medical, farming, trucking, sanitation, and power plant employees are dead will we really be up shit’s creek.
Is it just me, or do others see the apparent lack of meaningful engagement by our Federal Govt. to do what is truly necessary to combat these problems too? Or is it purposeful denial? I think what we’re seeing is the culmination of multiple chains of events visited up the US populace to actually do harm. Why else would tens of thousands of illegal immigrants crossing the Southern border with an assortment of diseases and ailments even be allowed entry, much less be quietly whisked off to undisclosed locations around the country and integrated into our society? I don’t think it is any coincidence that hundreds if not thousands of primarily children are coming down with a heretofore rare virus in the US, but has been raging through the population in Central America? Is it a coincidence that these children are co-mingled with the children brought in from Central America and placed in our schools? I think not, but then I’m one of those Tin Hat Conspirators.
So is it just another coincidence that the head of the CDC appears to be a bumbling, clueless fool who continually not only downplays the seriousness of Ebola being visited upon our shores, but also gives us patently false information regarding the spread of Ebola?
Like everything else our government has told us for the past decade or more, we continue to be lied to and mislead on EVERY major event that either directly or indirectly affects our lives these days.
When the puppet Obama told us five days before the election of 2008 that the was going to “fundamentally change the United States of America” even the most skeptical of us had no idea of the scope of that transformation. But we’re getting a full dose of it now aren’t we?
Dutchman-“Have the Army Corps of Engineers build some Popeye’s Chicken Shacks. Then we air drop chicken and watermelons as a humanitarian effort. “….and the Colt 45
“….and the Colt 45″ and two zig zags.
Typhoid Mary 1906
Ebola Barry 2014
Did a lot of reading on Ebola last night including several studies…..it apears to me based on the studies that Ebola could be an airborne virus.
We need to immediately cancel all visas for people coming from ebola-stricken countries. Few planes fly directly to the US from those countries, and canceling flights won’t do much, since they can travel through other countries – as Duncan did. Anyone coming from Africa needs a visa to enter the US. They won’t even try to get here if they know they’ll be turned back. Doing this will only slow the onset of Ebola growth in the US by about six weeks, which might be enough time for a vaccine to be mass-produced, although probably not. This could be far worse than most of us have contemplated. Hope that Russian vaccine is real.
Administrator says: Extrapolation is a wonderful technique. Is this a chart of the U.S.?
Lol …….You better hope not
Admin – The Vox chart appears to be mainly a West African plus world estimate through November, extrapolated on a doubling of new cases every 22 days.
How bad could the Ebola outbreak get? There are lots of predictions floating around. The World Health Organization projects that 20,000 people will be infected through November. HeathMap, put the number at about 14,000 if there’s no improvement in the situation. VOX
West Africa could see up to 10,000 new Ebola cases a week within two months, the World Health Organization said Tuesday, also confirming the death rate in the current outbreak has risen to 70 percent. CBS
http://www.vox.com/cards/ebola-facts-you-need-to-know/what-is-the-ebola-virus#E6723144
MIA –
DaPerfessor – Vot duz dis meen? MIA –
MIA –
Your second para has math consistent with the current best-fit equation I developed back in beginning of September so, it sniffs about right to me.
The predictions in para 3 kinda go off the rails though. The same equation takes us out to January of 2017 before seeing that kind of infection rate.
But, remember that equations are just that… they are not reality nor great at predicting the future. At some point, all epidemics burn themselves out. And, specifically, a type of epidemic that causes such visible symptoms burn themselves out sooner rather than later. The uninfected desert the scene of infectious particles. That limits spread and potential fatalities. (Now, if this suddenly has mutated to be insect-borne, all bets are off.)
The bigger problem here is the economic one….
Want to see folks desert airplane travel? Just keep on doing what the “experts” are allowing.
Want to see the income statements of hospitals crash? Ditto.
More than 1 or two cases at almost any “capable” (or believed to be so) hospital will swamp the resources available. As a corollary, anybody with an IQ above that of an over-ripe cabbage will avoid going to a hospital – – for anything. (In reality, almost anything except trauma care is “elective” under such circumstances.)
At some point, the hysteria being allowed to develop could easily lead to people avoiding most public places perhaps even right into the workplace.
DaP
Sorry about the mis-post, MIA. I have no idea what happened!
DaP
DaPerfessor – The x2 & 22 day extrapolation appears to be what the WHO and HealthMap are using in their calculations. Utilizing the same formula I’m getting about 65,000 cases by the end of the year and over a million by April if it doesn’t burn itself out in the before then.
This hopefully may be a reasonable estimate for a third world country without out good medical facilities. What is going to the impact when this ebola stuff breaks out and sweeps through in India, China, Indonesia, South & Central America and Mexico. The economic loss and loss of human life could be in billions of $ and lives..
MIA –
The current math suggests only about 30,000 cases by then. It could be wrong, I’ll admit.
What I do not see is the disease “sweeping” anywhere. Localized infection foci with subsequent burnout. Cases in each focus could get to between 5-10K before people being to leave the area or avoid contact with it.
Remember that it got to Lagos, Nigeria back in July?
It seems to already have been stopped, if not slowed considerably.
Seems to me that metroplexes on other continents should be able to as well. Infection in smaller, isolated regions will be self-limiting. (I’m not being cold, that is just the math of outbreaks.)
When it comes to infectivity, ebola is not influenza, measles or the plague. What captures the emotions is the nastily visual symptoms.
No question that I agree that economic loss will be huge. For that to happen, all that needs to be done is for the media to keep pumping the story out of perspective.
Not hiding yet,
DaP
Kill Bill: My son is an aviation technician with an avionics certification. He does much the same thing every day. He’s highly trained as you are, and in the excellent physical shape the job requires as you were/are also I assume. There is inherent danger and then there is carelessness. The two shouldn’t be mistaken.
I have been in medical services since 1994. First as an EMS person then as a nurse. I am used to putting my life on the line in service to others. I used to be the one who ran into the burning house you all ran out of. I’ve fallen through floors, been in flashovers, broken bones from collapsing gear, been puked on by contagious patients, been stuck by contaminated broken glass, had exposures to tuberculosis, meningitis and hepatitis among other things. It is part of the job. You just keep working, whiners need not apply. HOWEVER.
I was trained in how to deal with all of the above, and I was given the tools to do my job properly and safely. My supervisors took my safety seriously. I was trained to recognize the symptoms/signs of danger in the situations I faced and encouraged – required even – to take appropriate action to minimize the dangers to myself and my crew.
This is not the case when it comes to Ebola. Hospitals aren’t capable of handling this, just ask any nurse or doctor in a facility near you – off the record, of course. There is no training and no real plans for training. No facility is going to waste the money to purchase the gear and then waste a lot of it in training staff how to safely don and doff it, unlike the training offered to me in HazMat, fire fighting, and EMS training. It’s just not going to happen.
You want people to not be afraid? Then they need to be trained to recognize early symptoms, to be ready to err on the side of safety, and to be aggressive about taking defensive actions. Nurses in particular are held up as these Florence Nightingales with lanterns sacrificing their lives in service to unwashed humanity (even the males among us).
Do you really think, when health care has become a multimillion dollar business, that image is going to be the reality? When what the WHO and the CDC say about transmissibility differs in not insignificant and potentially deadly ways? When Sanjay Gupta can’t doff protective gear without contaminating himself on live TV?
My husband also works in the health care field and had a conversation with a doctor about Ebola. The doctor said straight up that if it became an epidemic he wasn’t going to be bothering to come to work, he was going to be home caring for the safety and health of his family where he belonged. That’s the reality. It’s not pretty, it’s not what the public wants to hear, but reality is a harsh mistress.
I’m not afraid, at least not blindly so. I think one must take precautions, and protect oneself, and be able to assess risk. I have a lot more chance of getting a Norwalk type virus than I do of getting Ebola, thankfully, because one involves 3 days of wishing I were dead and one involves the likely possibility I will in fact die. It’s all in assessing risk.
DaPerfessor – Missed your Lagos & Nigeria July posts. With no extensive mathematical or medical background in microbiology, my spreadsheets were ginned up the other night to try and get a line on what is going on with this virus and it’s potential spread. They are in no way guaranteed to be representative of the current or future elboa spread of the disease. My spreadsheet calculations for 30,000 elbloa cases comes in on November 27, 2014, if that figere is off, I may have to borrow your program to keep up to date.
If this disease can be contained in localized areas and die out in a short period of tine, with minimal loss of life in West Africa or other third world locations with minimal outbreaks in the rest of the world all will be well.
The thing to possibly be concerned about is if this ends up spreading other to third world countries with a total population of about 5 billion residents worldwide and only 10% or 500 million of the population contract the disease. 250 million will die with the present third world mortality rate of approximately 50%.
If it gets out of control here in the US and only 1% of the 340 million population contracts the disease, 3.4 million sick people will soon overwhelm our present unprepared medical system and facilities. Many will be left without medical care as Susan above and Hope ZK on a previous post have mentioned.
An occurrence if this nature would have a major impact on the economy and disrupt life for many here in the US Europe and other developed nations. Within the next 30, 60, 90 days there should be enough reliable information out there to make an accurate prediction on which way this outbreak will go.
MIA –
In the “disruption” that you note lies the end of propagation of infection. It will happen well before 1% infection rate. It seems to me that just 3-4 cases per large city would swamp hospital capacity to manage it. (You have to imagine the logistics for handling just the waste material coming out of the isolated room plus the real demands for effective decontamination. Not to mention availability of moon suits.)
We agree on the huge effect this could have on the economy. We differ on the threshold level at which such damage could occur. I aim at a much lower target for it to happen.
BTW – – notice something about infections so far? There’s two criteria, just satisfy one:
a. Native of the indigenous hot zones. OR
b. Health care worker for a case of “a” OR
c. Health care worker for a case of “b”
We have yet to see case of someone with casual exposure in the developed world getting sick. Time will tell, I guess.
Bottom line, I reckon most folks bodies are far safer than their wallets at this point.
DaP
Meant to say “two criteria with a variant..”
Going for more coffee!
DaP